Heart disease in women is the leading cause of death worldwide. Yet many still believe it is a “man’s problem.” This myth has delayed diagnosis and treatment for decades.
Why Heart Disease in Women Is No Longer a ‘Male Problem’: A 2026 Wake-Up Call
Introduction
Heart disease in women is the leading cause of death worldwide. Yet many still believe it is a “man’s problem.” This myth has delayed diagnosis and treatment for decades.
Today, the data tell a different story. Heart disease in women is rising across all age groups. Younger women are also at risk.
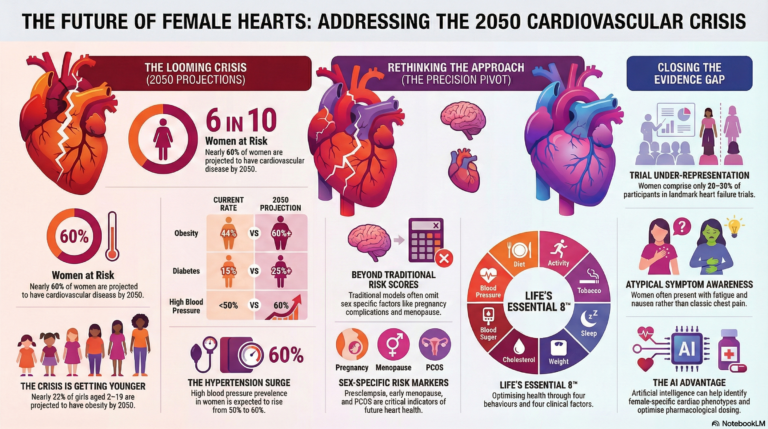
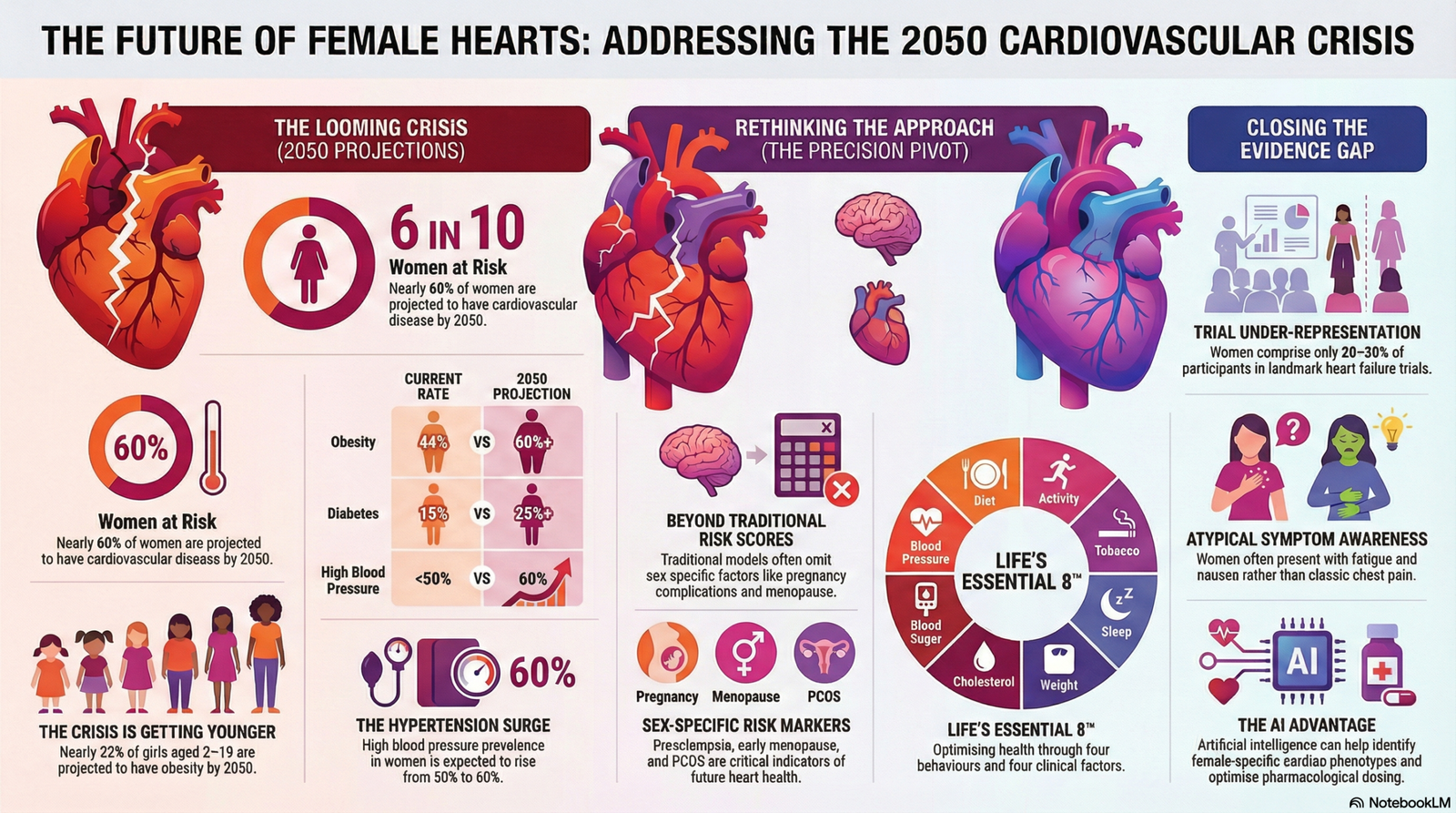
New projections warn that by 2050, nearly 6 in 10 U.S. women may live with some form of cardiovascular disease. That includes high blood pressure, heart failure, and coronary artery disease.
This article explains:
- Why heart disease in women is increasing
- How symptoms differ from men
- Female-specific risk factors
- The role of stress and mental health
- Practical prevention strategies
Understanding these differences can save lives.
The Shift from a “Male Problem” to a Global Female Health Crisis
For decades, heart disease was framed as a male illness. Research studies mostly included men. Treatment guidelines were built around male symptoms.
That approach left women behind.
Now, heart disease in women is recognized as a major public health crisis.
Startling Statistics for the 2050 Horizon
Current models predict a sharp rise in cardiovascular risk among women.
By 2050:
- Nearly 60% of women may have high blood pressure
- Around 60% may live with obesity
- More than 25% may develop diabetes
These three factors alone greatly increase the risk of heart disease in women.
High blood pressure damages arteries. Obesity increases inflammation. Diabetes accelerates vascular injury. Together, they create a dangerous cycle.
Recognizing the Impact on Younger Generations and Girls
The rise is not limited to older women.
Nearly one-third of women aged 20–44 may develop cardiovascular disease within the next 25 years. This trend is alarming.
Childhood obesity also plays a role. By 2050, about 32% of girls aged 2–19 may live with obesity.
Early weight gain increases lifetime exposure to high blood pressure and insulin resistance. That sets the stage for heart disease in women later in life.
Prevention must start early.
The Rising Economic and Social Burden
More than 62 million women in the United States already live with cardiovascular disease.
The economic cost exceeds $200 billion per year. This includes hospital care, medications, and lost productivity.
Beyond money, the social impact is huge. Many women are caregivers, workers, and family leaders. When heart disease in women increases, families suffer.
This is not just a medical issue. It is a societal issue.
Why Women’s Heart Disease Symptoms Don’t Follow the “Male Pattern”
One major reason heart disease in women goes undetected is symptom differences.
Most people imagine a heart attack as crushing chest pain. That image comes from studies in men.
Women often present differently.
Moving Beyond “Typical” Chest Pain
Chest pain can occur in both sexes. However, in women, it is less predictive of blocked coronary arteries.
Some women have coronary microvascular disease. This affects small vessels and may not show on standard angiograms.
Because the pattern differs, diagnosis can be delayed.
Subtle Warning Signs: Fatigue, Nausea, and Jaw Pain
Women are more likely to experience:
- Extreme fatigue
- Shortness of breath
- Nausea or vomiting
- Indigestion
- Neck, jaw, or upper back pain
These symptoms may appear days before a heart attack.
They can be mild or vague. That makes them easy to ignore.
If symptoms are new, severe, or persistent, urgent evaluation is necessary.
The Danger of Misdiagnosis
Studies show women are more likely than men to be discharged from emergency rooms without full cardiac evaluation.
Their symptoms are sometimes labeled as anxiety, stress, or gastrointestinal problems.
This delay can be fatal.
Recognizing atypical symptoms is critical in reducing mortality from heart disease in women.
Female-Specific Risk Factors: Why Heart Health Is Different for Women
Women face unique biological risk factors that men do not.
These include reproductive health conditions, hormonal changes, and autoimmune diseases.
Reproductive Health: Pregnancy, PCOS, and Gestational Diabetes
Pregnancy is often described as a “stress test” for the heart.
Complications such as:
- Pre-eclampsia
- Gestational hypertension
- Gestational diabetes
are early warning signs of future cardiovascular disease.
Women with these conditions have a higher lifetime risk of heart disease.
Polycystic Ovary Syndrome (PCOS) also increases risk. PCOS is linked to insulin resistance, obesity, and metabolic syndrome.
These factors strongly contribute to heart disease in women.
The Menopause Transition
Before menopause, estrogen offers some vascular protection.
Estrogen helps maintain flexible blood vessels and favorable cholesterol levels.
After menopause, estrogen levels fall sharply. As a result:
- LDL cholesterol rises
- Blood pressure increases
- Central weight gain becomes common
This shift explains why cardiovascular risk increases rapidly after menopause.
Heart disease in women often becomes more apparent in the post-menopausal years.
Autoimmune Conditions and Chronic Inflammation
Autoimmune diseases are more common in women.
Conditions such as:
- Systemic lupus erythematosus
- Rheumatoid arthritis
increase cardiovascular risk.
Chronic inflammation damages blood vessels. It accelerates plaque formation.
Women with autoimmune disorders require aggressive cardiovascular risk screening.
Overcoming the “Yentl Syndrome” in Female Cardiovascular Care
The term “Yentl Syndrome” describes a troubling reality.
Women are more likely to receive proper cardiac care only when they present like men.
This bias has shaped decades of under-diagnosis.
A History of Gender Bias
For years, women were underrepresented in clinical trials.
Many landmark heart studies in the 1980s and 1990s included mostly men.
As a result, treatment protocols were designed around male physiology.
Heart disease in women was not fully understood.
Today, researchers are working to close this gap.
Closing the Representation Gap
Modern clinical trials now aim for balanced enrollment.
Sex-specific analysis is becoming standard practice.
Guidelines increasingly recognize that women may require different diagnostic thresholds and treatment approaches.
This shift is essential for improving outcomes.
Precision Medicine and AI
Emerging tools are promising.
Precision medicine integrates:
- Genetic data
- Biomarkers
- Lifestyle factors
Artificial intelligence can analyze patterns that traditional methods miss.
AI-based imaging and risk calculators may improve early detection of heart disease in women.
Technology must support equity.
Psychosocial Factors and Lifestyle Strategies for Women
Biology is not the only driver.
Psychosocial stress plays a strong role in heart disease in women.
The Impact of Stress from Multiple Roles
Women often juggle work, caregiving, and household duties.
Chronic stress raises cortisol levels. This increases blood pressure and inflammation.
Marital strain and caregiving burden have been linked to higher cardiovascular risk.
Stress management is not optional. It is preventive medicine.
The Mental-Heart Link: Depression and Anxiety
Depression is twice as common in women as in men.
It is also an independent risk factor for heart disease.
Depression affects:
- Physical activity levels
- Sleep quality
- Medication adherence
Anxiety disorders may increase heart rate and blood pressure.
Integrated mental and cardiovascular care improves outcomes.
Taking Control with “Life’s Essential 8”
Prevention remains powerful.
The American Heart Association highlights eight key targets:
Four health behaviors:
- Healthy diet
- Regular physical activity
- Adequate sleep
- Avoiding tobacco
Four health factors:
- Healthy weight
- Controlled cholesterol
- Stable blood sugar
- Normal blood pressure
Up to 80% of heart disease is preventable through lifestyle changes.
Heart disease in women is not inevitable.
Practical Steps Every Woman Should Take
Awareness must lead to action.
Here are simple but powerful steps:
- Know your blood pressure
- Check cholesterol regularly
- Screen for diabetes
- Maintain a healthy waist circumference
- Exercise at least 150 minutes per week
- Prioritize sleep
- Seek help for depression or anxiety
If you had pregnancy complications, inform your doctor. That history matters.
Advocacy starts with asking questions.
Conclusion: Advocacy Is the Best Medicine
Heart disease in women is no longer a male problem. It is a distinct and growing health crisis.
Women experience different symptoms. They face unique risk factors. They often encounter diagnostic bias.
But the future can change.
Early screening, lifestyle intervention, and equitable research are powerful tools.
Every woman should:
- Know her numbers
- Listen to her body
- Seek evaluation for unusual symptoms
- Advocate for thorough care
Heart health is not optional. It is essential.
FAQ: Common Questions About Heart Disease in Women
Why was heart disease long considered a “male problem”?
Early cardiovascular research focused mainly on men. As a result, doctors viewed heart disease as a male condition. This led to under-diagnosis in women.
What are the most common heart attack symptoms for women?
Chest pain is common. However, women often report fatigue, nausea, shortness of breath, and jaw or back pain.
Can pregnancy affect long-term heart health?
Yes. Conditions such as pre-eclampsia and gestational diabetes increase the risk of future cardiovascular disease.
What is Yentl Syndrome?
Yentl Syndrome describes the bias where women receive proper cardiac care only when their symptoms resemble the typical male pattern.