Public health officials track rising measles cases in Western North Carolina.
Measles Cases Rise in Buncombe County Amid Outbreak Concerns: A Scientific Analysis
Measles is currently spreading through Western North Carolina at an alarming rate. This virus is one of the most contagious diseases known to modern science. Since late December, seven cases have been confirmed across the state, with the majority concentrated in one area. In this report, you will learn why measles cases rise in Buncombe County and the scientific factors driving this local outbreak. We will examine clinical symptoms, molecular surveillance, and the long-term biological impact on the human immune system.
The Buncombe County Outbreak: Current Epidemiological Data
As of mid-January 2026, health officials have confirmed that measles cases rise in Buncombe County, which now accounts for five of North Carolina’s seven confirmed infections. These cases involve two unvaccinated siblings and are largely linked to an ongoing outbreak in South Carolina’s Upstate region. One case in Rutherford County remains an outlier because no source of exposure has been identified.
High-Risk Environments in Candler
A primary point of concern for researchers is the Asheville-Pisgah Christian School in Candler. One of the infected children attended this facility. State records indicate that only 41.4% of students at this school are vaccinated against measles. This is significantly lower than the 95% threshold required to maintain community immunity.
Statistical Tracking and Community Spread
The North Carolina Department of Health and Human Services has launched a new dashboard to monitor these trends. This tool provides updates twice weekly on case counts and exposure locations. While health officials have not yet confirmed widespread community transmission, the potential for a larger outbreak is high due to low vaccination pockets.
Clinical Presentation: Identifying Measles Symptoms

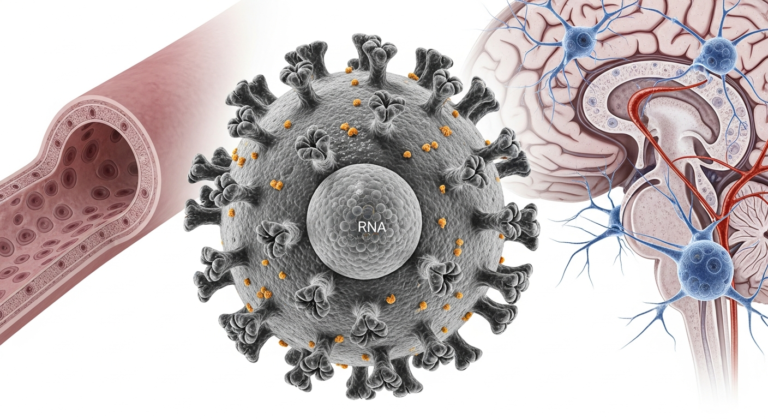
The measles virus (MV) is an airborne pathogen that travels through respiratory droplets. It can remain suspended in the air for up to two hours after an infected person has left a room. For those unprotected, the risk of infection is near 90% if exposed.
The Initial Incubation and “Three Cs”
Symptoms usually appear 7 to 14 days after a person comes into contact with the virus. The first signs are typically high fevers, which can exceed 104°F (40°C). Patients also exhibit the classic “Three Cs”:
- Cough (often described as a barky cough).
- Coryza (runny nose).
- Conjunctivitis (red, watery, or bloodshot eyes).
Diagnostic Markers: Koplik Spots and Rash
Two to three days after the first symptoms, Koplik spots may appear. These are tiny white spots with red backgrounds found inside the mouth. Finally, the signature red, blotchy rash begins to descend from the hairline. It spreads over the face and neck before moving down the trunk to the arms, legs, and feet.
Pathophysiology: The Threat of “Immune Amnesia”
A critical reason for concern when measles cases rise in Buncombe County is the virus’s ability to “reset” the human immune system. This phenomenon is known as immune amnesia. It is a unique characteristic of the measles virus that extends far beyond the initial rash.
Destruction of Memory Cells
The virus targets Signal Lymphocytic Activation Molecule (SLAM) receptors found on memory T-cells and B-cells. These cells are the body’s “strategists” that remember past infections. Measles infects and destroys these cells, effectively wiping out the body’s immunological memory of other diseases.
Long-Term Vulnerability
After recovering from measles, a patient is immune to the virus itself. However, they become highly vulnerable to secondary infections like pneumonia or influenza. Research suggests it takes approximately 27 months for the immune system to rebuild its previous protective memory.
Professional Opinion: In my view, the threat of immune amnesia is the most overlooked risk of the current outbreak. When vaccination rates fall below 95%, we are not just risking a week of fever. We are risking years of increased mortality from other preventable diseases in our children.
Molecular Surveillance: Advancements in Genomic Sequencing
As measles cases rise in Buncombe County amid outbreak concerns, scientists are using advanced tools to track transmission. Standard epidemiological investigations often struggle to differentiate between transmission chains during large outbreaks.
Direct Sequencing from Clinical Samples
Recent studies have developed methods to sequence complete measles genomes directly from patient urine samples. Using filtration and nuclease treatments, researchers can remove background human and bacterial DNA. This allows for high-resolution molecular mapping of how the virus moves through a community.
Identifying Transmission Chains
Complete genome sequencing provides more detail than older methods that only looked at partial gene segments. This data helps public health authorities understand if cases are imported from international travel or linked to local clusters. It is vital for identifying exactly where community spread is taking place.
Mitigation and Prevention: The MMR Vaccine

The MMR (measles, mumps, and rubella) vaccine remains the primary defense against rising cases. Since its introduction, it has led to a 99% reduction in measles cases in the United Kingdom and United States.
Vaccine Safety and the Autism Hoax
Concerns regarding a link between the MMR vaccine and autism are based on a fraudulent 1998 study. This study, authored by Andrew Wakefield, manipulated evidence and involved undeclared conflicts of interest. It was fully retracted in 2010, and multiple large-scale studies involving millions of children have found no link between the vaccine and autism.
Protective Protocols
- Two Doses: A complete series is 97% effective at preventing infection.
- Post-Exposure Prophylaxis: Receiving the vaccine within 72 hours of exposure can prevent disease in some cases.
- Immune Globulin (IG): For infants or pregnant women, IG can be given within six days of exposure to reduce severity.
Severe Complications and Mortality Risks
Measles is often misunderstood as a minor childhood illness. However, when measles cases rise in Buncombe County, the risk of severe medical complications increases proportionally.
Acute Complications
Approximately 1 in 5 unvaccinated people in the U.S. who catch measles require hospitalisation. Serious risks include:
- Pneumonia: Found in 1 in 20 children and is the most common cause of death.
- Encephalitis: Occurs in 1 in 1,000 cases and can lead to permanent hearing loss or intellectual disability.
- Death: 1 to 3 out of every 1,000 children infected will die from respiratory or neurologic issues.
Rare Long-Term Fatality: SSPE
Subacute sclerosing panencephalitis (SSPE) is a fatal disease of the central nervous system. It develops 7 to 10 years after a person has recovered from the initial measles infection. While rare, it is almost always fatal and results directly from the original measles virus lingering in the body.
Public Health Strategy: Contact Tracing and Isolation
Health departments use specific guidelines to manage outbreaks when measles cases rise in Buncombe County.
The 21-Day Quarantine
Because the incubation period can last up to 21 days, exposed individuals without proof of immunity must quarantine for three weeks. This prevents the virus from spreading further if they become symptomatic.
Seeking Medical Evaluation
If you suspect exposure, you must call your healthcare provider before visiting. Clinics must prepare the environment to prevent infecting other vulnerable patients. Healthcare workers often use N95 respirators or fit-tested masks to protect themselves during these encounters.
Mathematical Modelling and Seasonality
Research shows that measles transmission follows seasonal patterns. Historically, cases tend to rise in the winter months, often modulated by school terms and holiday gatherings.
Susceptibility Reconstruction
Scientists use case reports to estimate “susceptibility fluctuations” in a population. By looking at historical time series, models can predict the likelihood of an outbreak before it starts. This allows public health officials to schedule supplementary immunisation campaigns at the most effective times.
Forecasting Risk
Linear extrapolation of susceptibility helps determine how long a population can go between large outbreaks. When the number of unprotected individuals reaches a certain “endemic average,” the risk of a major community flare-up becomes critical.
Conclusion: Maintenance as a Task
As measles cases rise in Buncombe County amid outbreak concerns, we must view disease elimination as an ongoing maintenance task rather than a finished goal. The recent surge highlights how quickly a “measles-free” status can be threatened when vaccination rates falter.
Professional Opinion: Our community stands at a crossroads. The current data from Asheville-Pisgah Christian School is a warning bell. Without an immediate increase in vaccine uptake, the biological reality of measles—its airborne efficiency and its ability to erase immune memory—will ensure this outbreak grows.
Frequently Asked Questions (FAQ)
Q: Is there a specific treatment or cure for measles?
A: No, there is no specific antiviral treatment or cure. Supportive care includes rest, fluids, and fever-reducing medication. In hospital settings, Vitamin A may be administered to reduce the risk of severe complications and mortality.
Q: Can you get measles if you have been vaccinated?
A: It is rare, but “breakthrough infections” can occur, especially in high-outbreak areas where the virus is heavily circulating. Approximately 10% of cases in some outbreaks are breakthrough infections, but these cases are generally much milder.
Q: How long is a person contagious?
A: A person is infectious from four days before the rash appears until four days after it starts.
Q: Who is at the highest risk for severe measles?
A: Children under age 5, adults over age 20, pregnant women, and people with weakened immune systems face the highest risk for complications.